Today, for a change, I'm writing something technical again. A topic that haunts me like a bad dream. For years. Again and again. Again and again. And again. Ever since my supplier once accidentally delivered so-called HME filters instead of simple dust and bacteria filters. These things seem to have a magical attraction, because they are unpacked at every opportunity and installed somewhere in my ventilation system. Even when I was still breathing through a mask, people tried to foist them on me. Although they are never used at all with mask ventilation. Totally absurd.
I am not an expert. I'm not a doctor either. But I can read. In this case, a 179-page document from the German Society for Pneumology and Respiratory Medicine (Deutsche Gesellschaft für Pneumologie und Beatmungsmedizin e. V.) with the great name S2k - Guideline Non-invasive and invasive ventilation as therapy for chronic respiratory insufficiency (Link here). And the manufacturer's manuals. However, their content is identical. And to anticipate this, the same physical laws apply in non-clinical intensive care as in clinical care.
Like this. What is an HME filter?
Another technical term that many people use without knowing its meaning. The abbreviation stands for Heat and Moisture Exchanger. Translated into German, it means something like heat and moisture exchanger. From what I have learnt from various manufacturers, there are quite a few different filter materials used. Some manufacturers work with foams, others with paper or cardboard-like materials. There are single-layer and multi-layer models, and even extra air-permeable versions for athletes (yeah, right). But the function is the same for all of them. They regulate moisture and temperature.
HME filters are not bacteria filters.
That was new. There are probably also combination filters, but an HME filter does not necessarily have to have an antibacterial effect. This also explains why, regardless of the scenario, all filters used should never be HME filters. A bacteria and pollen filter must always be used directly on the machine. There are other reasons for this, such as the different resistance with regard to the permeability of breathing gases. But I find the bacteria thing easier to remember.
Now that I'm in such a good mood, let's clear up two more prejudices. What does the HME filter do again? It regulates heat and humidity in the event that the body can no longer do this and there is no active humidification with controlled heated and humidified breathing gas. That's another typical Paddy sentence, my goodness. Put simply, the nose, mouth and throat are normally responsible for regulating the heat and humidity of the air we breathe. But if someone sticks a cannula in your chest and steals your humidifier, you need an HME filter. If you're not really convinced, you can find everything on pages 28 et seq. of the guideline. Let's assume that I'm not talking rubbish, so let's establish two things.
A mask-treated patient does not need an HME filter. He never has. He doesn't. They never will, as long as nobody slits their throat, as happened to me. They breathe through their nose, mouth and throat with a mask. What's the point of an HME filter?
We have already disproved the second prejudice without realising it. Of course, we don't need an HME filter at home either. The pollen filter is fitted to the machine anyway, as already explained. And we do have active humidification on the cannula.
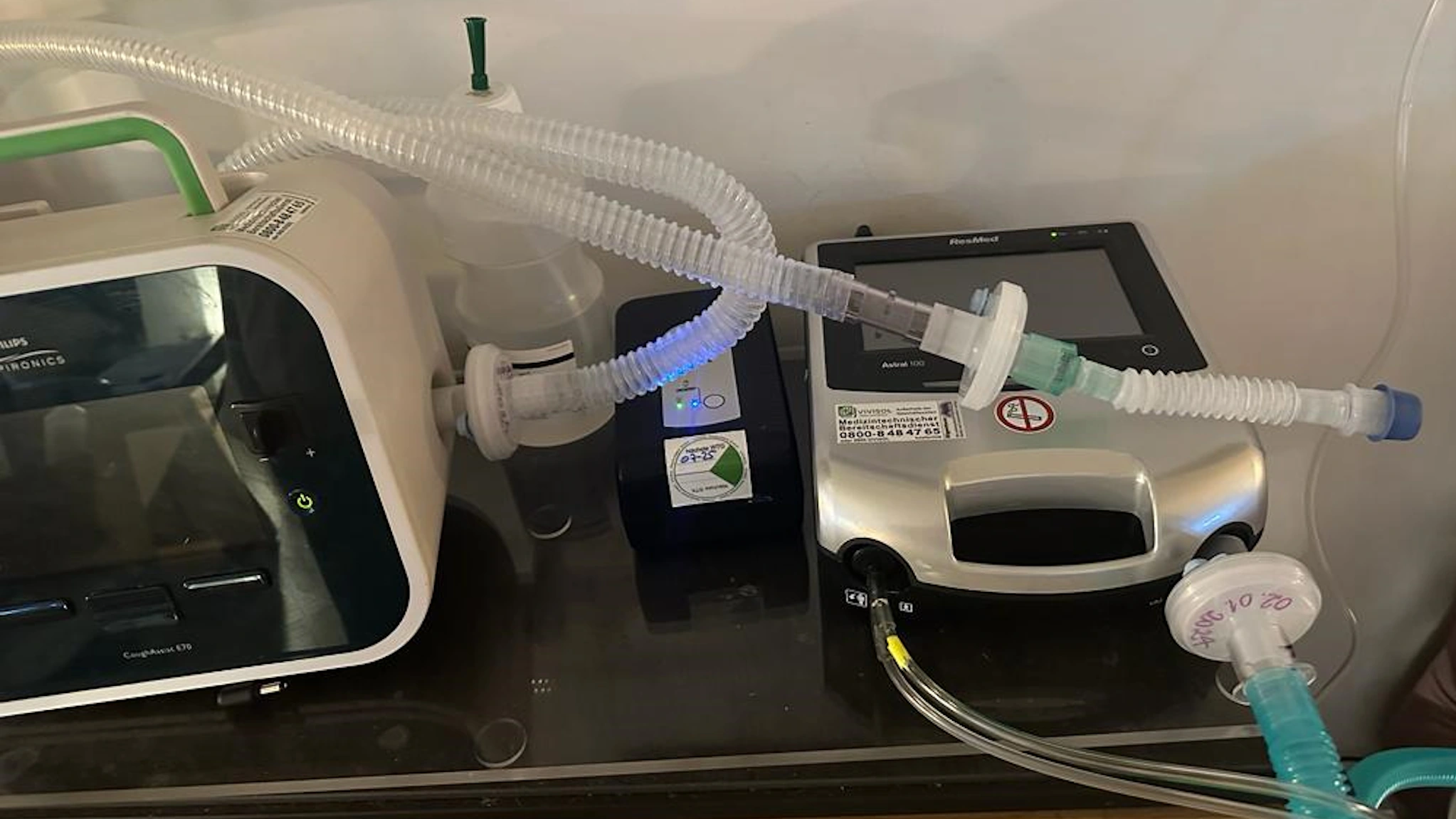
Only when there is no humidification is a dry hose and HME filter used. For example, when replacing the machine, during transport to hospital, ... well, in my case I can't think of anything else. But even in this case, there is a conventional bacteria filter on the machine itself.
And for the sake of completeness, it should be mentioned that in my case of invasive ventilation and normal mucus production, bacterial filters and a straight goose gargle should always be used on the cough aid. Because... oh, if you don't believe me, read pages 88 to 109. Seriously, I had enough other things on my to-do list for today, but this is really exciting. It also specifically deals with ALS and out-of-hospital intensive care. No-one would be surprised to have had a look at it.
Am I seeing something wrong? Let me know in the comments below.