It has been quite a while since I had problems with my health insurance. Since I have had a personal contact person who is able to understand the many, often only small, but practically always very special circumstances and conditions of ALS diseases, things are going well.
At least in theory.
Unfortunately, even my usual case handler is on holiday at some point. Or she is replaced, perhaps because she is at a training course. Or she is ill. It's supposed to happen in the best families.
And the ALS patient is already confronted with pointless discussions that are simply not necessary. A little more tact would really not hurt one or the other.
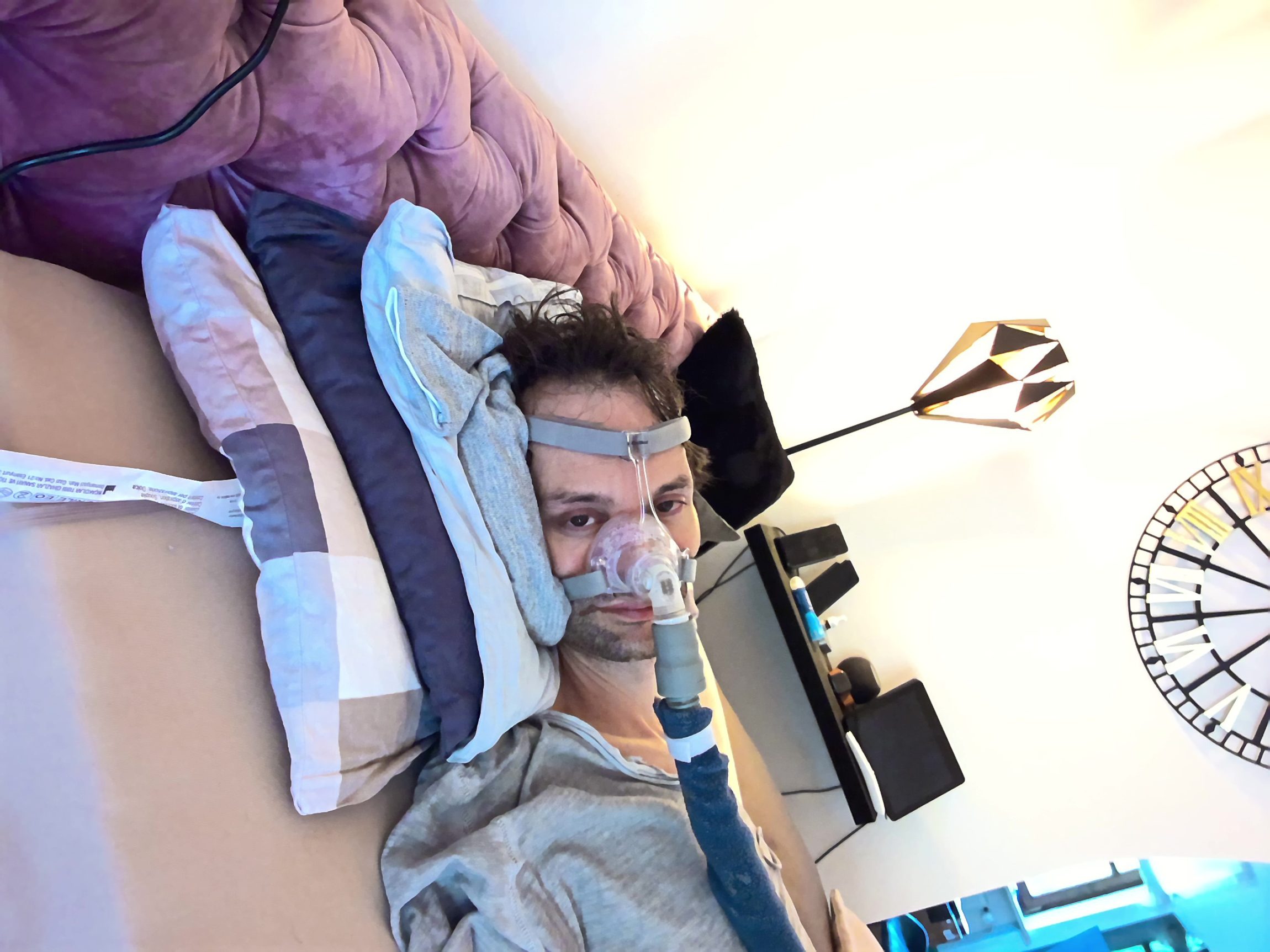
The NIPEG - Non-Invasive PEG
The thing is. I regularly choke on my own saliva when I'm not stored or not stored properly. Likewise if the humidifier is not refilled. Especially when I sit up, the secretion, which is stickier than usual in these cases, slips into my respiratory tract and causes me to cough. If only I could still do that.
Strictly speaking, this is not swallowing at all. That's always misinterpreted. I guess I mean that you can only choke on something that you had somewhere in your mouth or something. I'm also talking exclusively about secretion here, explicitly. not of food. But good.
What I'm getting at is that I'm probably less likely to choke on food compared to any healthy person because we're all always highly concentrated when we're eating. We even turn the music down. And if it does happen, the suction catheter and coughing assistant are right next to me. Since my new nursing service, all the nurses have even received instruction in the devices. This was not the case with the two intensive care services before, although as far as I know it was required by law.
The really big problem with eating is that my muscle strength in my mouth and lips is just not there anymore. I can't get the food through the straw into my mouth. And that's where the creative solution comes into play, which I can only recommend to anyone affected to try out. Provided, of course, that swallowing as such still works.
Take a PEG syringe with an ENfit connection, mount an Easybag transfer system on it and cut it in half. The non-invasive PEG is ready, as I have affectionately named it after my NIV (non-invasive ventilation).
There's no such thing as can't. Sure it is.
I have been feeding myself this way since the beginning of the year. The guys from my new care service are responsive to me, take the time I need.
If I have a lot of slime or spill - which was the standard a month ago because I was regularly positioned incorrectly or not at all - they work with me to find a solution instead of always postulating that I need a PEG and a tracheostomy tube. That really pissed me off at my old nursing service, when nurses constantly interrupted me or didn't even let me get a word in edgewise, but bothered me with their smart-aleck wisdom. Sure, as a non-intubation-capable ALS high-risk patient I should have non-essential operations without even weighing up the pros and cons beforehand. But you, the nurse, are so afraid of a statistically millionfold and millionfold significant and indisputable harmless Corona vaccination that you refuse it and even risk your job for it. On the one hand at least consistent, on the other hand a complete idiot, sorry. Everyone may make their own decision in this matter. But you are not even wearing out of respect for me a mask. You expect me to trust your medical advice? What do you dream about at night?
But let's take professionally behaving nurses as an example. That is, those who don't even sleep so soundly on day duty that they don't notice the ventilation alarm for over half an hour (unfortunately, this has happened more times than I could count). Then, yes, things look different. Then it works perfectly. I may quote from one of my messages to the cashier:
The staff at my new care service, which has been running for four weeks, are highly motivated and committed. They take the time I need. My daily dose via the injection: 5x high-calorie, protein-rich drinkable food with 400kcal each, intended for exclusive nutrition, 8-10 coffees or espressos, a small glass of water (40-50ml) after each coffee and food, tea, juice, wine or cocktails in the evening depending on my mood and visitors. In other words: if I pump any more into my stomach, I'll vomit from the other star.
E-mail to the AOK justifying my request dated 1.9.2022
I dare say that I wouldn't be able to manage more than a PEG either.
Quite simply because with 2,000 kcal a day just from drinking food - everything else, such as freshly squeezed fruit juices or the sugar from a minimum of six coffees, comes on top - I have reached the limit of what my body can tolerate.
I would also consider it unwise to exceed the daily dose recommended by the manufacturer even more than I already do.
Well, anyone who knows me and my writing style will already have an idea of what this amounts to. That's exactly what the desk jockeys at the AOK are now demanding of me.
Order for aids leads to request for surgery
Yes, that's how it can work when people who don't know what they're talking about are in control. Of course, the AOK refuses to cover the costs of the injections and the transfer systems. I have to admit that I myself have a borderline view of the latter, and I'd like to be fair about it, since it's well known that we're cutting them up. Incidentally, I would have understood that as a reason for refusal and accepted it without any further questions.
For which I can muster no understanding at all - neither factually, nor professionally, nor legally and a fortiori not human - are "reasons for refusal" of the following kind. I put them in inverted commas because they have nothing to do with my order. It's just know-it-all, stupid drivel.
According to the nursing report, you are already known to be underweight and should necessarily eat more calories, which you cannot manage with the sip feed and a transfer system from enteral nutrition.
E-mail from the AOK dated 31.08.2022
What? The ALS patient who has to live with paralysis and exclusively disease-related muscle loss (no malnutrition, dear health insurance clerk, go to a follow-up training) in the lower extremities on the right side, then on the left side, trunk, upper extremities on the right side, then on the left side and finally shoulder, neck and now jaw and cheek muscles, in other words, a person without muscles, of all people, is supposed to be underweight?
That's something.
But that is not enough. Science and the pharmaceutical industry have been looking for a solution since the 1980s. The good woman at the cash desk has long since pulled the solution out of the drawer:
Therefore, we recommend that you insert a gastostoma using a Stomabutton, which is also smaller than a PEG tube.
E-mail from the AOK dated 31.08.2022
So a PEG helps against my muscle atrophy caused by decay of the motor nervous system. Yeah, no, that's clear. For ALS patients. Worthy of a Nobel Prize.
Keep in mind that this medical advice comes from someone who has never spoken to me, never seen me. Who doesn't even know my medical records, let alone have a clue about what it means to live with ALS. Who relies on an expert opinion of the MDK, which was prepared without even asking me. It was drawn up by people who expect that my state of health will - again quote (!) - not deteriorate in the future.
I pull myself together and remain factual. I expect only one explanation from the lady. Where on earth is the difference in calories if I eat the food via PEG instead of taking exactly the same food and amount orally? I really don't understand it. I'm actually a pretty smart guy. I thought so.
The health insurance company answers the question as follows:
I am sorry that we were unable to provide you with a satisfactory solution to your initial enquiry. For this reason, we would urgently recommend that you contact your treating doctor regarding your diet and your underweight in order to find a satisfactory solution together with him or her.
E-mail from the AOK dated 01.09.2022
I don't know, can that be considered an admission? I read between the lines something like "I have no idea how a PEG is supposed to build your muscles, but that's what it says in our support guide". Let's face it, any Indian call centre (to weave in a bit of cliché) would have reacted more professionally.
But the main thing is to refuse and beat the helpless patient. And is anyone still surprised that health insurers have such a bad reputation?
As far as the matter with the doctor is concerned, I don't deny that I should do this if I haven't already done so. But I have already done so. Much more than that. On this point, too, Ms Vorschnell should have done her own research before coming up with such ridiculous statements. Because:
- I am in weekly contact with my family doctor. He is well informed and even approves of my food intake solution.
- My speech therapist checks my swallowing every week. She is totally enthusiastic about my variant with the syringe. In fact, she even tries out some procedures on herself first, and then with her other patients (I'm thinking, for example, of the topic of water versus tea, or speaking in the supine position).
- I already talked to my neurologist at the Friedrich-Baur-Institute of the Großhadern Hospital (FBI, a world-renowned and recognised institution for the treatment of neurodegenerative diseases such as ALS) about a year ago. As soon as the first swallowing problems occur, I should contact them and I will get an appointment in two to three days.
I wouldn't be me if all this information wasn't naturally available to the health insurance company. In writing, of course.
All the doctors and therapists treating me, even my speech therapist, are constantly writing reports for the insurance company. The last one was either from my neurologist from the practice at Prinzregentenplatz, who confirmed the necessary need for respiratory masks, or from my speech therapist, who determined that I can no longer speak well in order to apply for a speech computer. It is absurd that so much ignorance on the part of insurers is always to the detriment of the often defenceless patient. At least as far as amyotrophic lateral sclerosis (ALS) is concerned, my insurance company is more ignorant than knowledgeable.
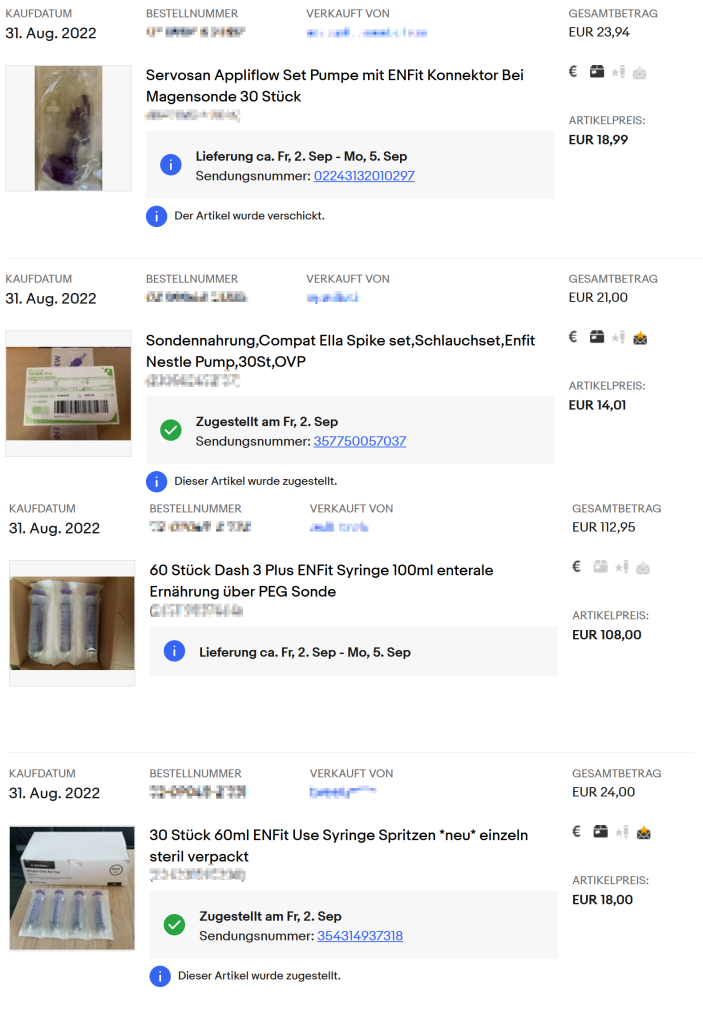
The pragmatic solution is called ebay
What can I say? I like to discuss. Very much so. But it's only fun at eye level. If something meaningful comes back. Conversations like these are idle and really spoil the whole week. I deal with it by writing about it. The positive encouragement I get back from you and from all of you strengthens me in what I do and how I do it.
Nevertheless, it still leaves a bad taste in my mouth to know that not every ALS patient is like me. Financially, too, I am probably the exception. It is always quite surprising that I am not exempt from co-payments despite my situation. I am all the more pleased to have a pragmatic solution for anyone similarly affected. The offer from my pharmacy used to look like this:
We already have some of the Enfit syringes in stock. Do you need them for a full payment? The total price of the syringes is 218,44€ (4x20ml, 3x60ml).
E-mail from my pharmacy dated 10.06.2022
Old steward. Pharmacy prices in all honour, but that doesn't even include the 100 ml syringes I need for eating. Only the ones for espresso and dental care are listed here, and even with my high coffee consumption, they would cost me more than the coffee itself. Sorry, even I say thanks, but no thanks.
Then I went back to ebay - no words: